
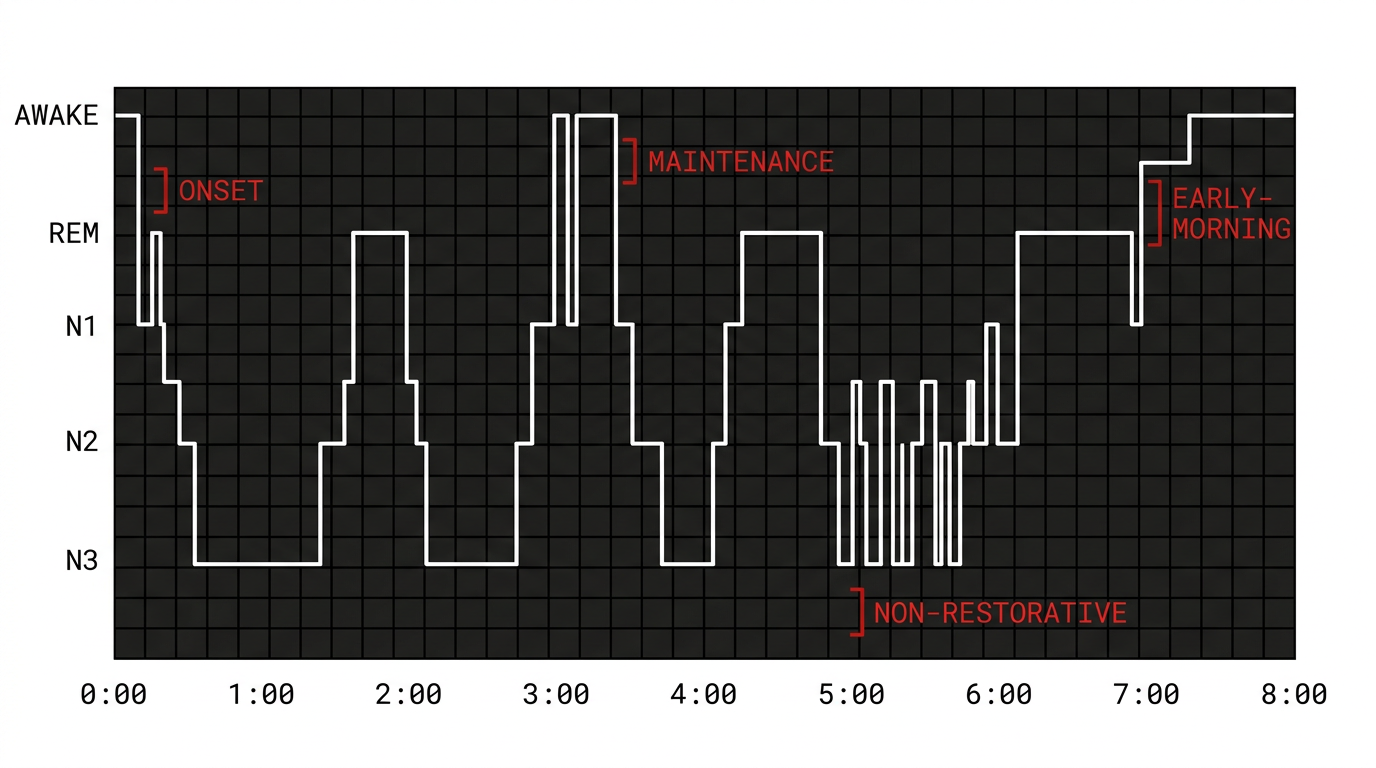
Onset insomnia
“My brain won’t turn off.”
You get into bed and the tape is still running. An hour passes, sometimes two. You watch the minutes go by.
Mechanismexpand_more
Onset insomnia is most often a problem of cortical arousal at the sleep-wake threshold. The systems that should be ramping down (sympathetic tone, cortical attention, the hypothalamic alerting signal) are still up. Melatonin timing can be misaligned, and the GABA-driven sedation that closes out the day is not engaging cleanly. The treatments that target this pattern are different from the ones that treat early waking.